







| 图片: | |
|---|---|
| 名称: | |
| 描述: | |
- Anterior Mediastinal FNA
Your questions are good and some require a long answer. If you are going to The Chinese Cytology Meeting this March in Guangzhou, that will be very beneficial to you, Dr. Zhao and I are both going. There will be a pre-conference Thyroid FNA work shop organized by 金域, it will pretty much answer all your questions in detail.
1, yes, thyroid FNA is one of the most common FNA samples seen here at US. I see an average 6-10 thyroid FNA a day here.
2, Well-differentiated follicular carcinoma is generally not a cytologic diagnosis. But, the majority of thyroid carcinoma are papillary carcinoma anyway.
3, you are right.
4, Many colloid nodules can be separated from follicular neoplasms with confident. 粉蓝医疗科技(杭州)有限公司官网入口 however cannot.
OK! I think that everybody agrees that this is a malignant germ cell tumor. The question is how to subtype it. The immunoprofile is not for typical seminoma and it fits more for embrynocarcinoma. But, the morphology favors seminoma. My colleague (he is a very good pathologist)signed this case out as "malignant germ cell tumor, unclassifiable", I am not entirely agree with him. The ponit is that if the clinical management is no difference, then it should not matter.
I also agree with Dr. Zhao that we hope that our Chinese cytopathologists will be more proactive to participate in discussions. We as american trained Chinese pathologists working in the US are usually very busy in our daily diagnostic work and we spend our time here on the web is because we want cytopathology in China will catch up sooner than later. Thanks all for participation.
I am surprised that now I gave you the biopsy and the immunostain results, I did not get much response. At least, I would like to know how you are going to sign-out this case???
Remember, sometimes in pathology, there is no absolute "right" or "wrong" diagnosis, it is very important to think outside the box and get the patient treated appropriately!
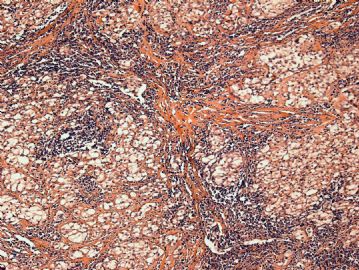 图1
图1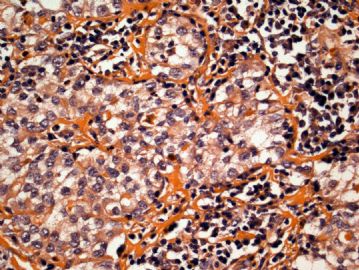 图2
图2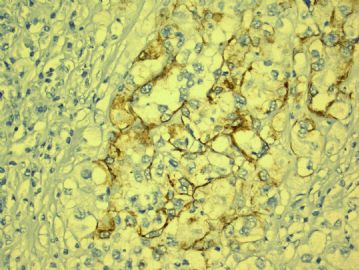 图3
图3 图4
图4
From the cytology, I think that everyone agree that it is malignant. The location of anterior mediatinum will let us think the following differential diagnosis: 1) Thymic Carcinoma; 2) Malignant lymphoma; 3) Malignant germ cell tumor; 4)Malignant thyroid carcinoma. I am glad that you are all considering the above possibility. But, remember that we most likely need immunostains to make a definitive diagnosis and sometimes, cytology has its limitation of not getting enough cells for cell block. So, in this case I asked for a biopsy. My colleague, Dr. Hansel, just brought the biopsy and a LOT OF immunostains to me. I just took some pictures and I am summarizing the immunostains:
Positive results: Only AE1/AE3 focally and CD30
Negative results: CAM5.2, TTF-1, CD20, CD45(LCA), ALK-1, PLAP, CD117,OCT3/4,bcl-2, p53, AFP.
Any thoughts on what this is?
Those are good differential diagnosis. This was a case I was on cytology service last week and the clinician did a FNA on this 3.5 cm anterior mediastinal mass. Patient has no history of other malignancy.
I had a similar differential as yours on the rapid read. I worried that the cell block will not be enough for immunostains, I suggest the clinician to do a biopsy. On the cytology, I favor a malignant germ cell tumor.
I will keep you posted on the follow-up.











